Initiation of ART reduces loss to follow up in HIV-TB co infected patients
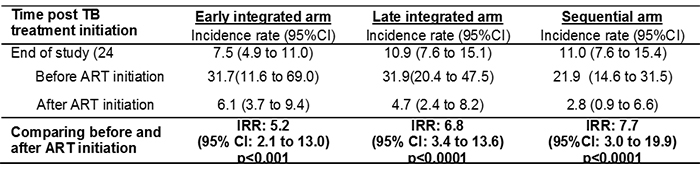
A secondary analysis on the CAPRISA 2003 SAPiT trial, which as-sessed the optimal timing for initiating antiretro-viral therapy (ART) in HIV-TB co-infected patients, shows that the incidence rates of loss to follow-up (LTFU) were not significantly different across the early integrated, late integrated and sequential trial arms (p=0.313). However, LTFU rates among TB patients initiating ART were dramatically reduced compared to those not initiating ART within each trial arm (Table). Rates of LTFU were 5.2; 6.8 and 7.7 fold higher before ART initiation compared to after ART initiation in the early integrated, late in-tegrated and sequential arms respectively.
The SAPIT trial previously demonstrated that ART initiation during TB therapy dramatically improves survival by 56%, and this analysis now demonstrates another added benefit of initiating ART during TB treatment by reducing LTFU in TB patients. The median time to LTFU among patients not initiated on ART was 2.8 (IQR: 0.5 to 6.7) months from TB treatment start.
These results increase the strength of the World Health Organisation’s recommendation of initiating ART within the first eight weeks of TB treatment, as ART initiation during TB treat-ment not only provides a survival benefit, but also confers a programmatic benefit of reducing LTFU among TB-HIV coinfected patients.
Table 1: Incidence rate of LTFU at different follow-up time points.